Dr. Todd Bovenizer presents treatment of a challenging asymmetrical Class II malocclusion utilizing Damon™ Q selective torques and early light elastics
 Compliance is paramount to a satisfactory orthodontic finish. Treatment results are only as good as the level of participation a patient provides. Specifically when determining what type appliance to employ for A/P correction, it is necessary to evaluate the psychological commitment each patient will likely exhibit.
Compliance is paramount to a satisfactory orthodontic finish. Treatment results are only as good as the level of participation a patient provides. Specifically when determining what type appliance to employ for A/P correction, it is necessary to evaluate the psychological commitment each patient will likely exhibit.
[userloggedin]
Good oral hygiene, negligible appliance breakage and debonding, and consistent elastics wear, if applicable, are all critical to an excellent result. Without compliance, treatment success is significantly lessened. In the following case, I demonstrate how a sound diagnosis and careful treatment planning can positively affect case development and the eventual outcome.
Orthodontists must evaluate each case with the end result in mind in order to select the proper torques that will achieve the desired result. Difficult Class II cases may also need A/P correction (with elastics or a fixed appliance, such as AdvanSync™), which determines incisor torque selection. I evaluate the malocclusion and skeletal pattern to determine which appliance is best suited to correct a Class II, taking into consideration my estimation of the patient’s proclivity for compliance. In this particular case, I surmised that compliance would be a non-issue, so I proceeded with an elastics-only treatment plan.
The Damon™ Q bracket system offers selective torque values that are vital for effective treatment planning. It is only through use of passive Damon™ System technology and its reduced friction would I treatment plan with only light elastics. Using light elastics that begin at bonding is kinder to tissues. Beginning A/P correction concurrent with leveling and aligning also speeds treatment time and allows me to start finishing mechanics much earlier, providing additional time to detail the occlusion when necessary. I also like to remain in stainless steel wires for 6 months for arch coordination and stability.
Case presentation: diagnosis
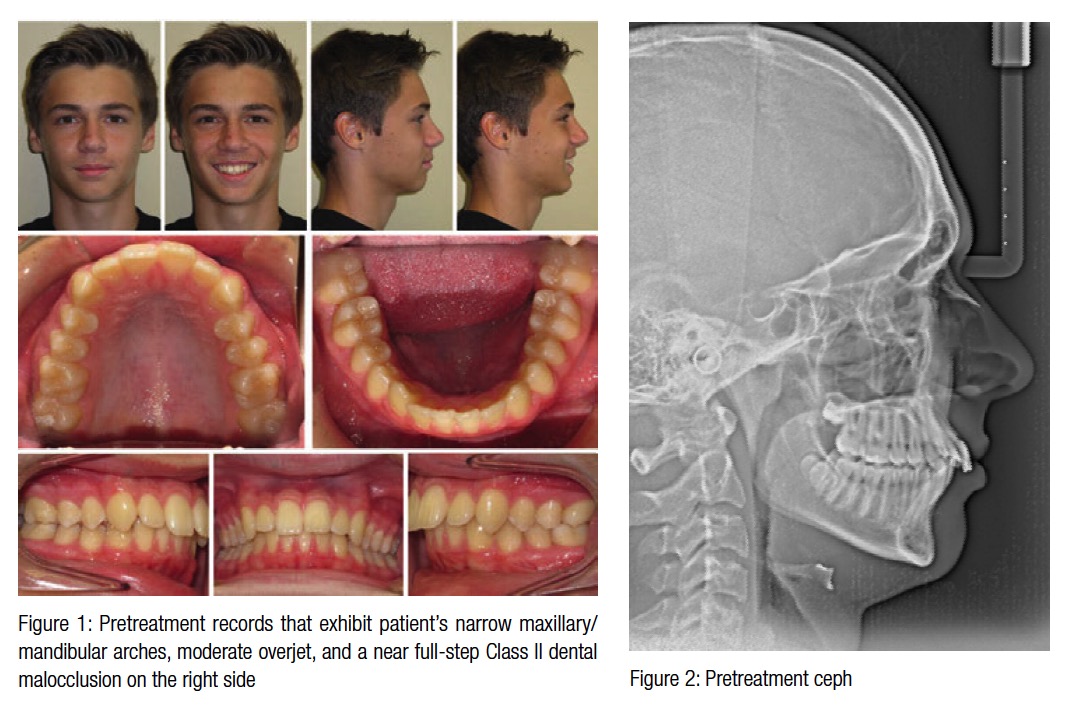
A 13.6-year-old adolescent male presented with no significant dental history, complaining that he did not like his smile or midlines. He exhibited a Class I skeletal relationship with narrow maxillary/mandibular arches, moderate overjet, and a near full-step Class II dental malocclusion on the right side (Figures 1-3).
Treatment plan
In assessing the case, I had a very important decision to make — whether to use elastics or a fixed Class II dental corrector. In my practice, this choice dictates torque selection because I pay particular attention to axial inclination of maxillary incisors. I determined that elastics therapy would be the right treatment plan choice in this case because the examination had gone well, and I anticipated compliance from both the patient and his parents.
It has been my experience that using fixed Class II correctors, such as Forsus™ or Herbst® therapy, results in retroclination of the incisors, which dictates high-torque incisor brackets. Given that I had decided to employ early light elastics therapy (beginning with 2 oz. elastics and progressing from there), I chose low-torque Damon Q self-ligating brackets U/L 2-2 and high-torque brackets for the U/L 3s. I would expand the buccal segments, coordinate the arch forms, and be careful to assess incisal angulation, the smile arc and transverse expansion at every appointment to ensure their proper development.
Treatment progress
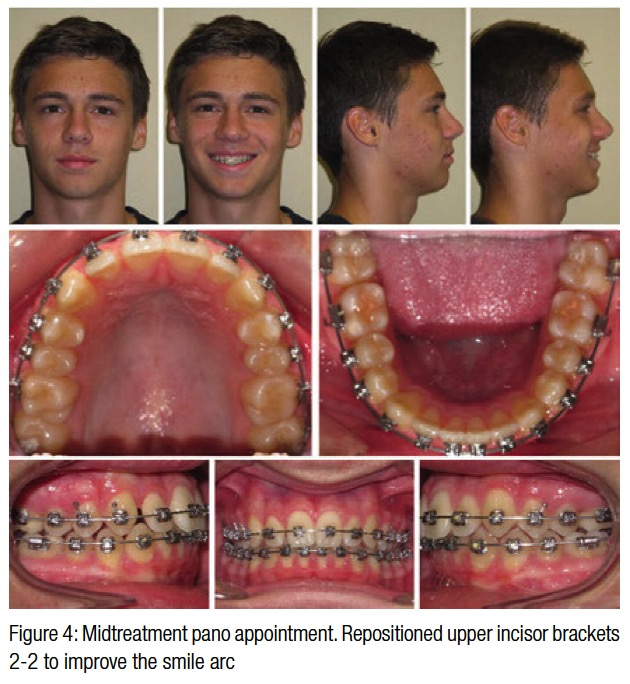 At the start of treatment, I indirect bonded the patient with Damon Q low-torque appliances U/L 2-2 and high-torque brackets on the U/L 3s. I placed Ormco’s .014″ Damon Copper Ni-Ti® wires and began short Quail 3/16″ 2 oz. Class II elastics (from Ormco) U4-L6, bilaterally, full time until 6 weeks prior to engaging the finishing wires. The patient remained on short Class II elastics for 16 weeks — the amount of time spent in .014″/.018″ round Copper Ni-Ti wires. At this point, I bonded the 7s, transitioned to rectangular .014″ x .025″ Copper Ni-Ti wires and began Parrot 5/16″ 2 oz. Class II elastics on the right side U3-L6, keeping the short Class II configuration (Quail 3/16″ 2 oz.) on the left side. After 10 weeks, I moved to .018″ x .025″ Copper Ni-Ti wires (upper and lower) and attached Bear ¼” 4.5 oz. elastics on the right side, continuing the Quail 3/16″ 2 oz. on the left side. After 8 weeks in these wires (at the midtreatment pano appointment), I repositioned the maxillary upper incisors 2-2 because his smile arc was flatter than desired, then specified nighttime only elastics wear with the same sizes/weights/attachments (Figures 4). To further develop the transverse arch and accommodate bracket repositioning, I left the .018″ x .025″ Copper Ni-Ti wires in place for 6 more weeks prior to engaging finishing wires. I make the determination about how long to leave the rectangular Copper Ni-Ti wires engaged on a case by case basis; I do not prescribe to a “one fits all” approach.
At the start of treatment, I indirect bonded the patient with Damon Q low-torque appliances U/L 2-2 and high-torque brackets on the U/L 3s. I placed Ormco’s .014″ Damon Copper Ni-Ti® wires and began short Quail 3/16″ 2 oz. Class II elastics (from Ormco) U4-L6, bilaterally, full time until 6 weeks prior to engaging the finishing wires. The patient remained on short Class II elastics for 16 weeks — the amount of time spent in .014″/.018″ round Copper Ni-Ti wires. At this point, I bonded the 7s, transitioned to rectangular .014″ x .025″ Copper Ni-Ti wires and began Parrot 5/16″ 2 oz. Class II elastics on the right side U3-L6, keeping the short Class II configuration (Quail 3/16″ 2 oz.) on the left side. After 10 weeks, I moved to .018″ x .025″ Copper Ni-Ti wires (upper and lower) and attached Bear ¼” 4.5 oz. elastics on the right side, continuing the Quail 3/16″ 2 oz. on the left side. After 8 weeks in these wires (at the midtreatment pano appointment), I repositioned the maxillary upper incisors 2-2 because his smile arc was flatter than desired, then specified nighttime only elastics wear with the same sizes/weights/attachments (Figures 4). To further develop the transverse arch and accommodate bracket repositioning, I left the .018″ x .025″ Copper Ni-Ti wires in place for 6 more weeks prior to engaging finishing wires. I make the determination about how long to leave the rectangular Copper Ni-Ti wires engaged on a case by case basis; I do not prescribe to a “one fits all” approach.
Finishing
At 10.6 months after bonding, the finishing wires were placed — U: .019″ x .025″ Damon stainless steel; L: .016″ x .025″ Damon stainless steel with Impala 3/16″ 6oz. elastics U3 to L4-6. I chose not to employ a TMA wire in the upper arch because I did not anticipate any wire manipulation and desired the transverse aspect of the arch form to develop even more fully. The stainless steel wires would remain in place for 5.6 months prior to debonding. We saw the patient for two more visits during this time — one for a retie and then the appointment 6 weeks prior to bracket removal to place 3/16” 6 oz. settling elastics, U3-L3-4 on the left side and U4-5-L4-5 on the right side.
Thanks to Dr. Stuart Frost (Mesa, Arizona) for the protocol of maintaining finishing wires for 6 months for adequate arch development and coordination. I always try to treatment plan with this time frame in mind, which helps case management when starting treatment with 7s erupted and with treatment time estimates.
Results
 Due to the patient’s exceptional response from both compliance and biological perspectives, the A/P was corrected using only light elastics begun at bonding. These mechanics negated the need for a fixed Class II appliance that can cause iatrogenic maxillary incisor retroclination. The variable torque brackets selected reduced proclination of the mandibular incisors and kept the maxillary incisors upright.
Due to the patient’s exceptional response from both compliance and biological perspectives, the A/P was corrected using only light elastics begun at bonding. These mechanics negated the need for a fixed Class II appliance that can cause iatrogenic maxillary incisor retroclination. The variable torque brackets selected reduced proclination of the mandibular incisors and kept the maxillary incisors upright.
I feel one of the most important aspects of beautiful treatment is not only a pleasing smile arc, but the proper inclination of the incisors. These are just two reasons why the Damon Q bracket is so helpful in treating cases. I feel I can gain control from the start of treatment, even during the round-wire phase.
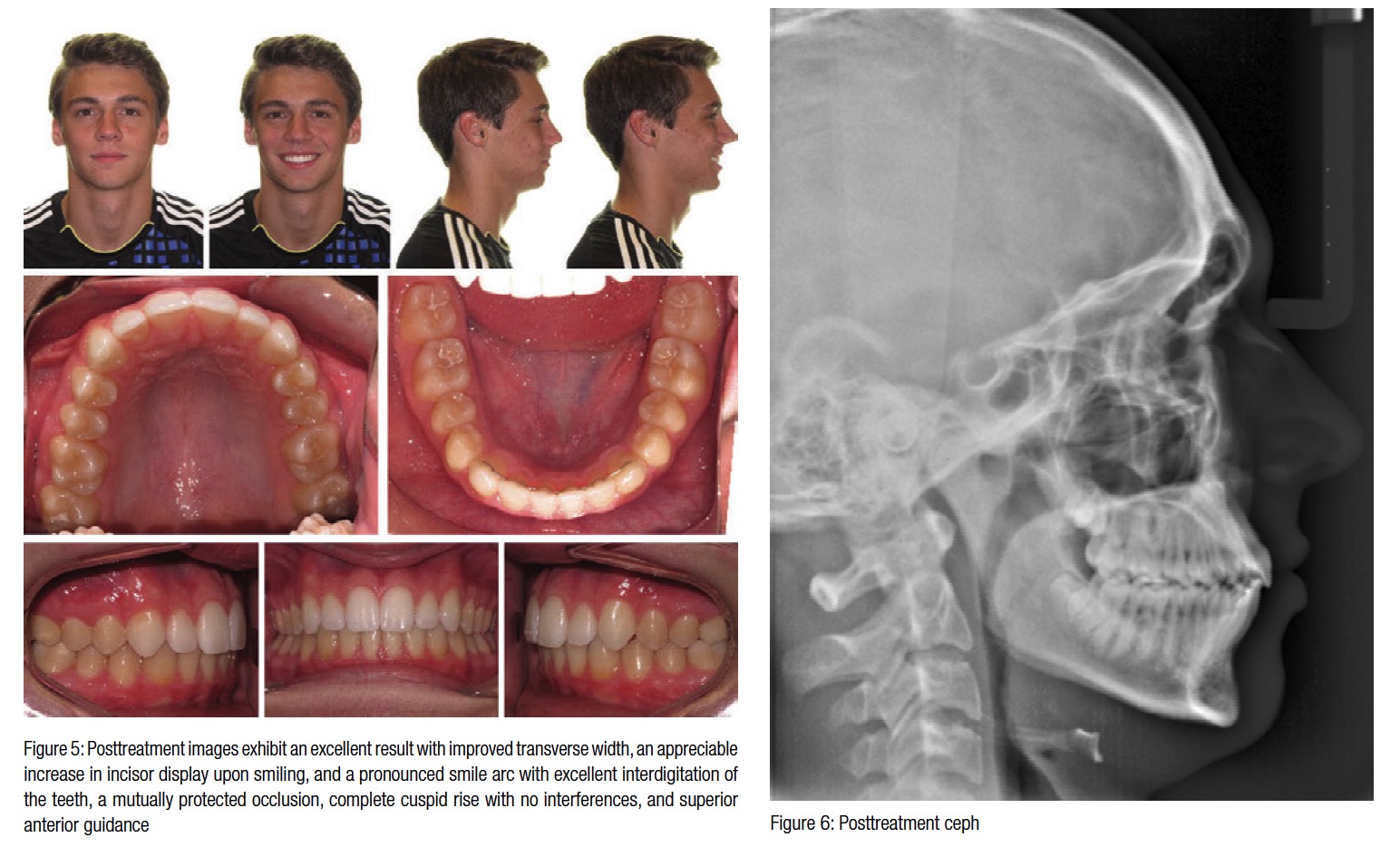
This patient’s arches rounded out nicely, and his buccal corridors improved dramatically. There was also an appreciable increase in his incisor display upon smiling and a pronounced smile arc with excellent interdigitation of the teeth. He finished with a mutually protected occlusion and complete cuspid rise with no interferences. He also now benefits from superior anterior guidance (Figures 5-7).
Conclusion
The key to this case was the diagnostic treatment planning and indirect bonding setup. I selected the incisor torque values based on the force patterns of the planned elastics. Had a different appliance been selected for A/P correction, different torque choices would have been made. I also positioned the brackets at the FA point (at the center of the clinical crown) and bonded the brackets from the posterior to the cuspids to take advantage of the “wedge effect” that Dr. Dwight Damon (Spokane, Washington) discusses, which dramatically improves smile arc design. Not every patient in my practice can commit to the level of compliance this patient did. Because he did so, the case finished in 16.2 months and 10 appointments (including bonding and debonding and one repair) rather than the 18-20 months it could easily have gone.
[/userloggedin]
[userloggedout][/userloggedout]
 Todd Bovenizer, DDS, MS, is a Diplomate, American Board of Orthodontics, recertified in 2010, who maintains a full-time practice in Cary, North Carolina. He serves as President of the North Carolina Association of Orthodontists and is also actively involved with many study clubs, locally and nationally. His practice has been selected as a test site for practice management software, and he participates in clinical evaluations to assess appliances in development. Dr. Bovenizer earned his DDS and MS in Orthodontics from West Virginia University.
Todd Bovenizer, DDS, MS, is a Diplomate, American Board of Orthodontics, recertified in 2010, who maintains a full-time practice in Cary, North Carolina. He serves as President of the North Carolina Association of Orthodontists and is also actively involved with many study clubs, locally and nationally. His practice has been selected as a test site for practice management software, and he participates in clinical evaluations to assess appliances in development. Dr. Bovenizer earned his DDS and MS in Orthodontics from West Virginia University.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
