






Welcome to Orthodontic Practice US
A dental journal and publication for orthodontists
Current Issue

4 ways to factor marketing into your practice management
Current Issue, Practice Management
Dr. Kyle Fagala and Kayla Hallen offer strategies to attract new patients When you think of practice management, what comes ...

Practice management in orthodontics
Current Issue, Product Profile
Dr. Michael Bicknell discusses an educational opportunity for building practice strategies In today’s evolving orthodontic field, effective practice management is ...

Weathering the storms
Columns, Current Issue
Lisa MolerFounder/Publisher,MedMark Media Droughts, heat waves, rain, hurricanes, blizzards, tornadoes, wildfires, and earthquakes, or beautiful sunshine — no matter where ...

The breathing-smile connection: the intersection of airway health in orthodontics
Concepts, Current Issue
Dr. William E. Harrell, Jr. offers some insights into the history, growth, and importance of airway health There is a ...

Integrating AI in dental practices
Current Issue, Practice Management
Gary Salman explains how to reap the benefits of AI more safely As artificial intelligence (AI) continues to permeate various ...

A bold decision in practice
Columns, Current Issue
Claudia Pinter, DMD “I want to improve my smile, but braces are not an option.” I hear this so often ...

DIBS AI
Current Issue, Product Profile
Dr. David Lowe Real-world experiences As the popularity of digital bonding using DIBS AI from OrthoSelect continues to grow, we ...

The custom approach to digital IDB
Current Issue, Product Profile
(And how it saves time and money) When Dr. Paul Trotter took over his father’s practice, he faced a big ...

Occlusal harmony: the final frontier in orthodontic excellence (Part 2)
Concepts, Current Issue
Dr. Gregori M. Kurtzman offers ways to preserve orthodontic outcomes Occlusion plays a pivotal role in determining the long-term success ...

Orthopreneurs Summit At Sea
Current Issue, Product Profile
A floating orthodontic think tank This past September, spared by the weather gods, orthodontists met on the high seas for ...

Precision with Spark™ Aligners
Current Issue, Orthodontic Experts
Dr. Claudia Pinter in her practice Dr. Claudia Pinter discusses an essential tool in her orthodontic practice As a young ...
Orthodontic Clinical Studies

An OMD assessment with TMD muscle pain: a case study
Clinical
Judith Dember-Paige, BSOHP, COM®, discusses how transformation sometimes takes years, but it’s worth the effort Stan was referred to my ...

The synergy of orthodontics and myofunctional therapy
Clinical
Dr. Maria Sokolina discusses a game-changer in long-term stability and sleep apnea treatment Abstract Orthodontic treatments often face challenges related ...

Conservative approach of fortuitously found odontoma in a child with severe autism
Clinical
Dr. Gabriela Aurora Asensi discusses treatment of a special needs patient Abstract A case of an unexpectedly found compound odontoma ...

Dental Mental Network
Clinical
Dr. Brett E. Gilbert and Sue Jeffries discuss the importance of providing a safe space in support of dentists’ mental ...

Practitioner perceptions of the link between orthodontics and temporomandibular disorders (TMD): a survey of dentists, orthodontists, and oral and maxillofacial surgeons
Clinical
Drs. Chadwick Augusty, Shadbeh Taghizadeh, Vincent Graves, John Stockstill, and Courtney McCracken (biostatistics) study the perceived association between orthodontics and ...

Examining the dental canon
Clinical
Drs. Francesca Scilla Smith and Larry W. White discuss centric occlusion, centric relation, and the role of canines Canines Prior ...

Into the unknown: emerging evidence regarding risks of aerosols in the dental office
Clinical
Dr. Maria L. Geisinger discusses likely modes of transmission for the virus that causes COVID-19 Aerosols created during dental procedures ...

Next-generation treatment planning
Clinical
Editor’s intro: Using combination treatment plans allows Dr. Adam Schulhof to approach appliances like menu options — let him whet your appetite ...

CEREC Ortho software — where do you send your scans?
Clinical
Editor’s intro: Dr. Patrik Zachrisson shows how CEREC Ortho is a very versatile software that has many uses apart from the popular ...

Let the celebrities help
Clinical
Editor’s Intro: Even Tom Cruise flashes an imperfect smile. Model wide-raging smile esthetics with celebrity photos. Dr. Donald J. Rinchuse discusses ...

The physics of Class II correction
Clinical
Dr. James J. Jasper discusses the efficacy of the Jasper Vektor® Appliance Introduction From the beginning of the modern ortho-dontic ...

Fixed and removable orthodontic appliance case study
Clinical
Dr. Andrew Wallace uses the principles of “smile design” for a patient seeking cosmetic improvement of his upper and lower ...
Orthodontic Case Studies
Digital treatment planning and precision orthodontic appliances
Dr. Jacquee Schieck avoided orthognathic surgery for this high school patient Introduction Orthodontists are trained in moving teeth and improving ...
Case Studies

Pre-restorative orthodontic treatment for worn anterior teeth
Dr. Jane Wright illustrates the clinical and esthetic concerns that drove the treatment plan for this patient Growing up in ...
Case Studies

Whiten, align, and shine: whitening with aligners
Dr. Brigham Stoker illustrates a combination of treatment over 4 years Achieving the bright, confident smile our patients desire can ...
Case Studies

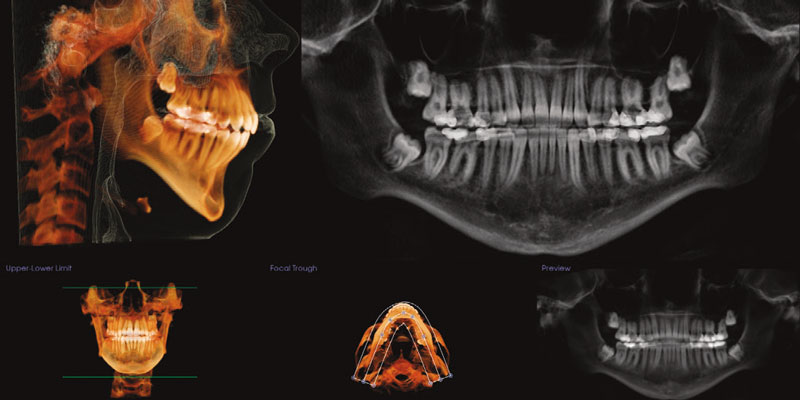
Strategic extraction patterns based on alveolar housing considerations using CBCT imaging: a case study
Drs. Jeffrey Miller and Claire Miclat show how CBCT can help an orthodontist plan more strategically Introduction When treating patients ...
Case Studies

Treatment of an adult Class II malocclusion with a hyperdivergent mandible and an open bite
Drs. Emad Hussein, Sari Amer, Yazan Ashhab, Khaled Qattawi, Mohammad Abo Mowais, Nezar Watted, Zuhir Anani, and Manal Samarah treat a ...
Case Studies

The power of choice
Dr. Manika Agarwal discusses relying on our strengths to develop a versatile approach The choice The prevalence of social media, ...
Case Studies

Pushing the limits
Dr. Jeffrey M. Heinz illustrates a clinical case study treated with Spark™ Clear Aligners In my practice, I have traditionally ...
Case Studies

Katelyn’s story
Figure 1: Katelyn Dr. Todd Rankin shares a story of extraordinary teamwork and the stunning transformation of a young woman ...
Case Studies

Anterior open bite correction in skeletal Class I patient
Dr. Diego Peydro demonstrates treatment for an open bite in seven appointments Introduction Over the years, there have been many ...
Case Studies

Using Spark™ Clear Aligners in open bite closure with TADs
Dr. Bill Dischinger illustrates treating a patient’s narrow arches and anterior open bite with clear aligner therapy My orthodontic training ...
Case Studies

Class II Division I, 9 mm overjet
Dr. Aron Dellinger discusses treatment with the Roncone PhysioDynamic System (PDS) application of the 20/20 molar bracket Initial impressions utilizing ...
Case Studies

Idiopathic condylar resorption: a case report
Dr. Bradford Edgren illustrates a patient with dysfunctional remodeling of the condyle A healthy 16-year 10-month-old female presented for a ...
Case Studies
Orthodontic Industry News
Angel Aligner™ Announces State-of-the-Art Manufacturing Facility in Greater Milwaukee
SAN CLEMENTE, CA, UNITED STATES, March 13, 2025: Angelalign Technology Inc. (HK:6699) (Angel Aligner™) www.angelaligner.com a global leader in orthodontic ...

EasyRx Expands 3D AI Services with Bleaching Trays and Sports Mouthguards
Industry News
ATLANTA, GA - [2/18/2025] - EasyRx, a leader in dental and orthodontic lab management software, has introduced two new features ...

LuxCreo Unveils 4D Bright™ Aligner, Simultaneously Enhancing Orthodontic and Aesthetic Dental Care
Industry News
Chicago, IL - LuxCreo, a global leader in personalized medical and dental devices, announced today the release of its latest ...

Oral Healthtech Startup Proclaim Expands National Dental Partner Network, Raises New Capital,and Adds Personal Health Industry Leader to Board of Directors
Industry News
Former Philips Personal Health CEO Egbert van Acht Joins Board of Directors Khosla Ventures, Global Asset Capital, Ensemble Innovation Ventures, ...
Great Lakes Dental Technologies Announces Certified Evergreen Recognition
Industry News
(Tonawanda, New York) Great Lakes is proud to announce completion of a meticulous assessment process to earn designation as a ...
Ultradent Donating to Southern California Fire Relief
Industry News
SOUTH JORDAN, Utah January 14, 2025. Ultradent Products, Inc., a leading developer and manufacturer of high-tech dental materials, is donating ...
Light Force Orthodontics Ranked 47th Fastest Growing Company in North America on the 2024 Deloitte Technology Fast 500™
Industry News
Achieves remarkable 2,985% growth, driven by commitment to personalized orthodontic care BURLINGTON, MA, November 21, 2024 - LightForce Orthodontics, makers ...

Solventum launches first 3D printed aligner attachments to revolutionize aligner treatment
Industry News
Clarity Precision Grip Attachments are fully cured, pre-loaded and precisely resemble the digital treatment plan after bonding (ST. PAUL, Minn.) ...

SureSmile Marks 30 Years of Innovation in Orthodontics
Industry News
As Dentsply Sirona's SureSmile celebrates its 30th anniversary, the journey of transforming orthodontics continues. SureSmile's pioneering innovations in hardware and ...

Georgia School of Orthodontics Honors Graduates of World’s Largest Orthodontics Residency Program
Industry News
Three-term Georgia Senator and renowned healthcare provider addresses graduates ATLANTA, GA (September 2024) -- Atlanta-based Georgia School of Orthodontics ...

Beautiful occlusion and stabile results with Early Orthodontic Treatment
Industry News
Early orthodontic treatment aims to detect malocclusions at an early stage and stop their development. The silicone eruption guidance appliance ...

New Study Explores the Efficacy of Photodynamic Therapy in Adolescents Undergoing Orthodontic Treatment
Industry News
Lund, Sweden - A groundbreaking clinical study titled "Efficacy of Regular Home Use of Dual-Light Photodynamic Therapy on Oral Health ...
